The paradigm of medical teaching in the medical training is that “SLE is a disease of females in the child bearing age group and the male to female ratio is 1:9”1. The present article is an attempt to compare the clinical profile of the rarer male SLE with female SLE which is more familiar clinical problem to a practicing physician.
Much of the data on the profile of male SLE comes from relatively small scale case series studies and the progile of oriental male sle patients is discussed in the present paper.
Why female SLE is commoner?
Estradiol binds to receptors on T and B lymphocytes, increasing activation and survival of these cells which are inappropriately activated by HLA and environmental factors as EBV to act hostile to autoantigens, thus favoring prolonged immune responses and prolonged tissue damages as in SLE. Testesterone was shown to have a protective effect the mechanism of which is poorly described in literature and needs further studies.
Differences in the clinical manifestations
Male SLE the commoner presentations are:
1. Pleurisy
2. Renal (kidney) disease(DPN Stage IV is commonest)
3. Thrombocytopenia
4. Seizures
5. Discoid lupus (reddish, scaly skin)
6. Subacute cutaneous lupus (skin lesions)
7. Hemolytic anemia (from the destruction of red blood cells)
8. Lupus anticoagulant (can promote abnormal blood clotting)
9. Drug-induced lupus erythematosus (DILE) due to greater incidence of diagnosis of systemic hypertension and arrythmia in males and its treatment with offending drugs.
10. Anti Ro Negativity which was statistically significant in many case series study.
Features common in female SLE
1. Neurologic (nervous system) symptoms
2. Alopecia (hair loss)
3. Thrombocytopenia (abnormal decrease in blood platelets)
4. Malar rash (rash on cheeks)Arthritis
5. Sjogren's syndrome (glandular damage that causes dryness of eyes and mouth)
Problems with Male SLE patients
Men with lupus face a unique challenge. It may be difficult for them to discuss a disease that so many people think occurs only in women. Because there are fewer men with systemic lupus, they may have trouble meeting other men with the disease. This may prevent them from gaining the benefits of mutual support. While many of female patients are interested in meeting any other people with SLE, virtually all of male patients ask about other men with whom they can speak.
References
1. Brauwnwald et al. “Principles of Internal Medicine 16th edition”;Tata McGrawhills publications.
2. Inman RD, Jovanovic L, Markenson JA, Longcope C,Dawood MY, Lockshin MD. Systemic lupus erythematosus in men: genetic and endocrine features. Arch Intern Med 1982;142:1813-5.
3. Steinberg AD, Melez KA, Raveche ES et al. Approach to the study of the role of sex hormones In autoimmunity. Arthritis Rheum 1979;22:1170-6.
4. Lahita RG. Sex steroids and the rheumatic diseases. Arthritis Rheum 1985^8:121-6.
5. Hazelton RA, McCruden AB, Sturrock RD, Stimson WH. Hormonal manipulation of the immune response in systemic lupus erythematosus: a drug trial of an anabolic steroid, 19-nortestosterone. Ann Rheum Dis 1983;42:155-7.
6. Lahita RG, Cheng CY, Monder C, Bardin CW. Experience with 19-nortestorone in the therapy of systemic lupus erythematosus: worsened disease after treatment with 19-nortestosterone in men and lack of improvement in women. / Rheumatol 1992;19:547-55.
7. Jungers P, Kuttenn F, Loite F et al. Hormonal modulation in systemic lupus erythematosus: preliminary clinical and hormonal results with cyproterone acetate. Arthritis Rheum 1985;28:1243-50.
Saturday, September 09, 2006
Wednesday, July 05, 2006
Journal review: Omalizumab in Asthma
What is Omalizumab?
It is a recombinant,humanized IgG1 monoclonal antibody that binds the IgE molecule at the same epitope on the Fc region that IgE binds the FcE RI receptor on the mast cells or basophils.
Mechanism of action
Ig E plays a central role in initiating bronchial asthma, by binding the allergen to specific receptors on mast cells to cause it degranulate. Omalizumab binds with the Fc portion of allergen laden IgE molecules and prevent it from binding to Fc receptor.
Projected indications
1. Asthma for atleast 1 year and on inhaled corticosteroids.
2. At least one positive allergen skin test.
3. Elevated IgE levels.
4. Patient with persistant asthma with coexistant allergic rhinitis, sinusitis and gastroesophageal disease.
Dasage: 0.016mg/kg wt/iu of IgE every 4 weeks subcutaneously. (aim is to reduce IgE <10 iu/ml)
Adverse effects
1.Epithelial and solid organ malignancies.
2. Anaphylaxis (paradoxical)
3.Rash,diarrhoea,vomiting,Epistaxis,menorrhagia, hematoma in injection sites.
It is a recombinant,humanized IgG1 monoclonal antibody that binds the IgE molecule at the same epitope on the Fc region that IgE binds the FcE RI receptor on the mast cells or basophils.
Mechanism of action
Ig E plays a central role in initiating bronchial asthma, by binding the allergen to specific receptors on mast cells to cause it degranulate. Omalizumab binds with the Fc portion of allergen laden IgE molecules and prevent it from binding to Fc receptor.
Projected indications
1. Asthma for atleast 1 year and on inhaled corticosteroids.
2. At least one positive allergen skin test.
3. Elevated IgE levels.
4. Patient with persistant asthma with coexistant allergic rhinitis, sinusitis and gastroesophageal disease.
Dasage: 0.016mg/kg wt/iu of IgE every 4 weeks subcutaneously. (aim is to reduce IgE <10 iu/ml)
Adverse effects
1.Epithelial and solid organ malignancies.
2. Anaphylaxis (paradoxical)
3.Rash,diarrhoea,vomiting,Epistaxis,menorrhagia, hematoma in injection sites.
Tuesday, July 04, 2006

Tuesday, May 16, 2006
Review artcle: Locked in Syndrome (Selectively De-efferented state)

Synonyms: Cerebromedullospinaldisconnection, Pseudocoma or de-efferented state.
Site of lesion
2. Basis pontis bilaterally sparing tegmentum.
3. Ventral aspect of medulla bilaterally sparing tegmentum.
Characteristics of the patient:
The patient is conscious, alert and awake as the tegmental ascending reticular activating system (ARAS) concerned with arousal is intact, so be careful with your bedside comments.
Blinking movements of the eyes are preserved; hence patient is able to communicate in a telegraphic pattern (“on or off” movements of eye lids).
Vertical movements are intact as it is controlled by the interstitial nucleus of cajal and the rostral part of the medial longitudinal fasciculus (MLF), which is situated in the tegmentum of the midbrain, which is spared in the locked in syndrome.
Horizontal movements of eyes are lost especially when the ventral part of the basis pontis is involved, leading to involvement of the 6th cranial nerve fascicle.
Patient may be aphonic because of the involvement of the corticobulbar fibers and motor nucleus of the lower cranial nerves especially the 7th, 9th, 10th, 12th cranial nerves.
Patient is quadriplegic due to involvement of pyramidal fibers in the lateral 2/3rd of cerebral peduncle of the midbrain or the basis pontis or the ventral aspect of the medulla.
“Fourier de prodromique” – Pathologically characteristic sudden onset of laugh at the onset of quadriparesis due to involvement of bilateral pyramidal system, producing psuedobulbar palsy like state before the onset of brainstem symptoms.
Etiology for locked in syndrome.
1.Lacunar infarcts.
2.Demeyelination(central pontine myelinolysis)
3.Haemmorhage.
4.Trauma.
5.Tumours.
Pseudo-Locked in states
1.Gullain barre syndrome
2.Acute polyneuritis
3.Myasthenia gravis
4.Poliomyelitis
References
1. Text book of neurology;Paul brazis.
2. National Institute of Neurological Diseases (NINDS) Reprot on Locked in Syndrome.
Sunday, May 14, 2006
CT corner: Schizencephaly

Schizencephaly is an uncommon disorder of neuronal migrational characterized by a cerebrospinal fluid–filled cleft, which is lined by gray matter. The cleft extends across the entire cerebral hemisphere, from the ventricular surface (ependyma) to the periphery (pial surface) of the brain.
The clefts may be unilateral or bilateral and may be closed (fused lips), as in schizencephaly type I, or separated (open lips), as in schizencephaly type II.
Presentation and outcome are variable, but patients typically present with seizures, hemiparesis, and developmental deficits. Usually, the severity of symptoms is related to the amount of brain affected by the abnormality.
References:
1.Barkovich AJ, Norman D: MR imaging of schizencephaly. AJR Am J Roentgenol 1988 Jun; 150(6): 1391-6.
2.Barkovich AJ: Schizencephaly. In: Pediatric Neuroimaging. 2nd ed. Philadelphia: Lippincott-Raven; 1996:219-25.
3.Barth PG: Schizencephaly and nonlissencephalic cortical dysplasias. AJNR Am J Neuroradiol 1992 Jan-Feb; 13(1): 104-6
Monday, May 08, 2006
Case Report: A Deadly Siren and an uncommon connective tissue disorder

Jithesh.k*, Shajith.S.*, Abhilash*, Hariprasad*, Shan** ,Geetha.P.** ,Benoy.J.Paul***.
Department of Internal medicine, Calicut Medical College.
(Published in CALFIM Journal)
Introduction
Of all the inflammatory myopathies the chance association with malignant lesions especially in the older age group is highest with dermatomyositis. However the extent of search that should be conducted for an occult neoplasm in adults depends on the clinical circumstances uncovered by the medical history and physical examination and not through an extensive blind search.
Case report
Mr........., a 48 year old previously healthy individual working in gulf countries with history of intermittent episodes of Bronchial asthma and Atopic features, presented in our outpatient department complaining of polyarthralgia involving predominantly the small joints of upper limbs and lower limbs symmetrically and generalized muscle pains for 1month and proximal muscle weakness of UL/LL and erythematous lesion of face of 3weeks duration .His physical examination showed no pallor, jaundice, cyanosis ,clubbing , edema or lymphadenopathy and pulse rate was 80/min,B.P.of 140/80 mm of Hg. His abdomen was soft with no hepatosplenomegaly or masses. Examination of chest and cardiovascular system was normal. Nervous system examination showed grade (4-) power of proximal muscles of upper and lower limbs, deep tendon reflexes were normal, with no sensory deficits, no cerebellar signs, Fundus -- normal with no overt features of peripheral neuropathy. . Locomotor system examination showed only arthralgia in the small, appendicular joints symmetrically predominantly of the upper limbs. Face showed an erythematous and edematous elevated lesions over the malar eminence on both sides involving the nasolabial folds and periocular and periorbital region, extending to the pinna on both sides.
In view of the presence of proximal weakness of the upper and lower limbs and the presence of a periorbital facial rash, the possibility of dermatomyositis was considered and we proceeded with investigations. Also a reasonable screening for occult malignancies was done to rule out secondary dermatopolimyositis.
Investigations
•Hb – 13.6 gm/dl
•TC – 7800 cells/mm3
•DC – P48 L 51 E1
•ESR – 39 mm/ I hr
•B.U. – 19 mg/dl
•S. Cr. – 0.41 mg/dl
•Na+ -- 140 meq/l
•K+ -- 4.3 meq/l
•CXR (PA) – WNL
•USG (abd) – Normal
•CPK – 7500 IU/L
•RA factor – Negative.
· Anti- ds DNA – Negative
· ANA – Negative.
Complete ANA profiling
•SS-A / Ro 52 – Positive.
•SS-B / La – Negative.
•Anti Jo -1 – Negative.
•Scl-70 – Negative.
•nRNP / Sm – Negative.
•Sm – Negative.
•CENP – Negative.
•AMA M2 – Negative
TFT
•T3 – 1.03 (0.86-2.02)
•T4 – 8.53 (5.13-14.16)
•TSH – 1.31 (0.27-4.2)
•Skin biopsy was done from the skin lesions
Showing epidermal atrophy. Epidermis shows occasional vacuolated basal cells with few scattered lymphocytes in the underlying dermis and mucinous change with an increase in the faint bluish matrix of dermis.
EMG was done to confirm with myopathic pattern of weakness, which showed spontaneous activity in the form of fibrillations and prolonged insertional activity with myopathic motor unit potentials suggestive of inflammatory myopathy.
Modified Bohan and Peter criteria were used to confirm a diagnosis of Dermatomyositis based on above clinical features and investigation reports.
Modified Bohan and Peter Criteria
.
1. Symmetrical proximal muscle weakness. (+)
2. Elevated muscle enzymes, (+)
3. Characteristic inflammatory myopathic EMG finding. (+)
4. Muscle biopsy showing evidence of inflammatory myositis.
5. Typical rash of Dermatomyositis (+)
(Three of the first Four + 5th criteria is needed for definitive diagnosis)
A reasonable screening for occult malignancies in the lung, GI system, testes and lymphoreticular system was done which was all-negative.
Patient was started on oral prednisolone at 40mg OD dose. Patient showed dramatic improvement in weakness and a decrease in CPK levels (4839 IU/l)
and skin lesion significantly decreased. Patient was kept under regular follow up to rule out any occult malignancy that may resurface in the future.
Photographs after treatment with steroids.
Discussion
Causes for Dermatomyositis
Primary
· Genetic predisposition (HLA DR3, HLA DQA1*0501).
Secondary
·
· Underlying malignancies (ovarian, breat, melanoma, colon, NHL).
·
· Autoimmune disorders (associated with MCTD or SS, rarely SLE Rhuematoid arthritis and Sjogrens syndrome).
·
· Infectious or toxic agents
· Drug-induced (implicated drugs include hydroxyurea, penicillamine, statins, quinidine, and phenylbutazone).
Treatment and follow-up of Dermatomyositis.
•Prednisone,
•Methotrexate,
• Azathioprine,
•Cyclophosphamide,
•Cyclosporin,
•Mycophenolate and
•High dose intravenous immunoglobulin.
•Diltiazem, a calcium channel blocker, may reduce calcinosis.
•Colchicine has also been reported to reduce calcinosis.
•Hydroxychloroquine may reduce the photosensitive rash.
•Avoid excessive sun exposure and use sun protection measures,
•Bed rest for those with severe inflammation of muscles,
•Physical therapy and activity to keep the muscles and joints moving.
•Raising the bed head for those with difficulty swallowing
•Most patients will require treatment throughout their lifetime,
•Completely resolves in about 20%.
· Treated DM has 5 year survival of ~95%.
•Specific Anti-Mi-1 is found in one quarter and
•Anti-Jo-1 in a few, usually those who have lung disease (80%).
•Patients who have disease affecting their heart (AV conduction abnormalities, DCM) or lungs (ILD), or who also have an underlying cancer do less well and may ultimately die from their disease.
References.
1. CALLEN JP: Dermatomyositis. Lancet 355:53, 2000
2. DALAKAS MC: Polymyositis, dermatomyositis, and inclusion-body myositis. N Engl J Med 325:1487, 1991
3. ARGOV Z et al: Various types of hereditary inclusion body myopathies map to chromosome 9p1-q1. Ann Neurol 41:548, 1997
4. ENGEL AG et al: The polymyositis and dermatomyositis syndromes, in Myology, AG Engel, C Franzini-Armstrong (eds). New York, McGraw-Hill, 1994, pp 1335-1383
5. IOANNOU Y et al: Myositis overlap syndromes. Curr Opin Rheumatol 11:468, 1999
Wednesday, May 03, 2006
Physical examnination: Vesicular breath sounds

Vesicular breath sound production
Classically the lung sounds were thought to be produced by the vibrations of the vocal cords and the proximal airways set in by the inspiratory movement of air, which is attenuated and conducted to the chest wall and the auscultating stethoscope by the normal air filled sacs called alveoli/acinus. The normal breath sounds were initially thought to be produced in the terminal air filled alveoli, and was called Vesicular sounds (Vesicle = small vessels). Present view is that the terminal airways including acinus are silent due to the laminar flow and low velocity of airflow,and breath sounds are solely producd by the vibrations of the proximal airways. As the vibrations of taut vocal cord can produce harmonics of both high and low pitches, and the normal vesicular breath sound is low pitched with a frequency of 16-200HZ, further supports the earlier proposed mechanism of attenuation and conduction of sounds by the terminal air spaces.
Definition of vesicular breath sounds
ATS definition of vesicular breath sound -- VBS is a low pitched rustling sound with a high intensity inspiratory phase which is continuous with a less intense and shorter expiratory phase, which normally extends to less than one third of inspiratory phase.
Now look at the first part of the diagram for the possible site of origin of each component of vesicular breath sound.
Look at the second part of the diagram for diagrammatic representation of normal vesicular breath sound (inverted and mirror image for better understanding).
Causes for decreased intensity of normal vescular breath sound.
1. Pleural effusion (Separation of conducting units from chest wall)
2. Pleural thickening (-do-)
3. Collapsed lung with occluded bronchus (Loss of conducting pathways)
4. Emphysema (Loss of laminar flow and low velocity airflow due to distended acinus)
5. Bronchial asthma (occlusion of conducting airways)
6. Thick chest wall (eg;Obesity)(separation of steth from the area of activity” lung”).
References
1. Kraman,SS: Vesicular(normal) lung sounds:How are they made,where do they come from,and what do they man?; Semi. In Resp Med 6:183,1985.
2. Forgacs,P: The functional basis of pulmonary sounds, Chest 73:399,1978.
Tuesday, May 02, 2006
Gastroenterology:Traube's space
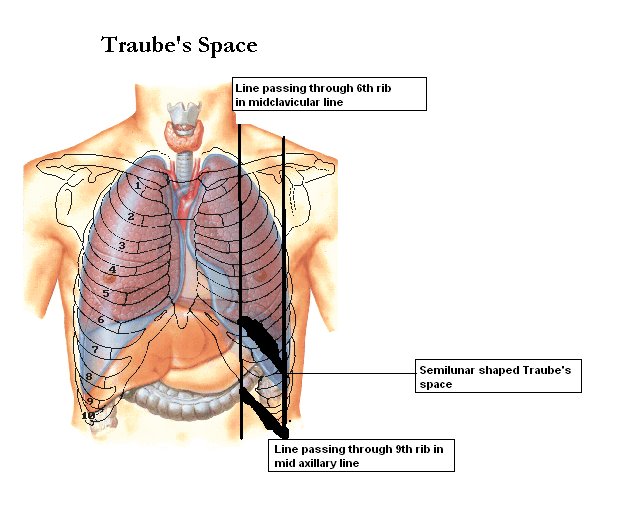
Surface Markings
1. Draw two vertical lines one passing through the 6th rib in the midclavicular line and the next passing through the 9th rib in midaxillary lines.
2. Now draw a smooth curving line with convexity upwards ftom the sixth rib in midclavicular line to 9th rib in midaxillary line.
3.Draw another straight line passing through the costal margin from 6th rib to 9th rib.
All these boundaries enclose a near semilunar space called Traubes space.
Anatomical boundaries are:
1. Right : Lateral margin of left lobe of liver.
2. Left : Spleen.
3. Superior : Resonance of lung.
4. Inferior : Costal margin.
Contents
1. Fundus of stomach (Hence percussion of Traubes area normally gives Tympanitic resonance).
2. Costo-phrenic recess of left pleura devoid of lungs.
Causes of obliteration of Traubes space:
1. Full stomach.
2. Left sided Pleural effusion.
3.Splenomegaly.
4. Enlargment ofleft lobe of liver due to any etiology.
5. Dextrocardia.
6. Proloiferative growth in fundus of stomach.
Note: A left lung mass lesion/consolidation alone never produces impairment as lung is not extending to traube's space.
Friday, April 28, 2006
Clinical signs: Rare signs of hypocalcaemia
.jpg)
A. Peroneal sign consists of dorsiflexion of foot and abduction of the toes on tapping the peroneal nerve on the lateral surface of the fibula just below the knee.
B. Erb's sign, or increased electrical excitability of the peripheral nerves to the galvanic current, was the most reliable proof of tetany in the days before blood chemical analyses were available. The procurement of electrical reactions is such a time consuming procedure that they are seldom sought for now.
C. Involvement of the autonomic nervous system has not been stressed in recent years as a manifestation of tetany but was well known to the older writers. They recognized as part of the picture of spasmophilia of infants disturbances of respiration; irregularity, tachypnea, an asthmatic type of breathing apparently due to bronchial spasm and even respiratory arrest as well as the better known laryngeal stridor.
D. Bradycardia, or more rarely tachycardia, and cardiac murmurs were noted.
E. Disturbance of the tonus of the gastrointestinal tract, manifested by abdominal distention, constipation or diarrhea, pylorospasm and vomiting were seen.
F. Pallor, erythema and urticaria were attributed to spasm of the capillaries of the skin. As a further possible sign of tetany, hemorrhages producing bloody vomitus, melena and hematuria should be mentioned.
References
1. J Stokes Jr. and K Dodd et al; Pediatrics, Dec 1948, 737-743, Vol 2, No. 6
Thursday, April 27, 2006

Wednesday, April 26, 2006
Review article: Pulsus Paradoxus(Reversed Bernheim sign)
Definition
The simplest definition of pulsus paradoxus is an exaggeration of the normal inspiratory decrease in systolic blood pressure. The current formal definition of pulsus paradoxus is an inspiratory fall of systolic blood pressure of greater than 10 mm Hg.
History
The reduction in pulse volume during inspiration was first described by Lomer in 1669 in constrictive pericarditis. A similar finding was described by Floyer and later by William in 1850 in bronchial asthma. Adolf Kussmaul (Freiberg, Germany) coined the term “pulsus paradoxus” in 1873 in three patients with constrictive pericarditis .Adolf Kussmaul in his 1873 manuscript ‘Ueber schwielge mediastinopericarditis und den paradoxen puls’ (Constrictive Pericarditis and the paradoxical pulse; ) described two important physical signs of pericardial disease: pulsus paradoxus and Kussmaul’s sign.
What is the paradox?
The paradox described by Kussmaul was a “pulse simultaneously slight and irregular, disappearing during inspiration and returning upon expiration” despite the continued presence of the cardiac impulse during both respiratory phases.
Others has described additional paradoxus in the same phenomenon that amidst the irregulary of the pulse palpated, the regularity with which the pulse disappeared during inspiration Moreover, another paradoxus was that the clinical method of assessment of this “pulse” is by measurement of the “systolic blood pressure”.
Methods of examination
1.Palpation(Clinical) :Usually, palpation of the central pulses (carotid) is recommended for the evaluation of the character of the pulse. However, pulsus paradoxus is better appreciated in the peripheral pulses (radial). When the pulsus paradoxus is severe, it may be possible to palpate a fall (reduction in the pulse volume) during the phase of inspiration and rise during the expiratory phase.
2.By Sphygmomanometer(Clinical): To measure the inspiratory decrease in systolic blood pressure, the cuff is first inflated 20 mm Hg above the systolic pressure, then deflated until the first Korotkoff sound is heard. Initially the Korotkoff sounds are heard only during expiration. The cuff is deflated until the Korotkoff sounds are heard equally well during inspiration and expiration. The pressure at which all the Korotkoff sounds are heard should be subtracted from the systolic pressure. If the difference between these two pressures is greater than 10 mm Hg, the patient has a pulsus paradoxus of a magnitude equal to that difference.
3.Pulse oximetry waveform analysis This technique has been found useful in the neonates with cardiac tamponade. In patients with obstructive airway disease since pulse oximetry is available in ICUs and emergency departments, it is a useful non-invasive means of continually assessing pulsus paradoxus and air trapping severity.
4.Arterial waveform analysisIn the intensive care setting, where the arterial waveform is available, pulsus paradoxus can be diagnosed by visualising changes in the systolic blood pressure tracing during the inspiratory and expiratory phases of respiration.
Causes of Pulsus Paradoxus
Cardiac causes
1. Cardiac tamponade2. Pericardial effusion3. Constrictive pericarditis4. Restrictive cardiomyopathy5. Pulmonary embolism6. Acute myocardial infarction7. Cardiogenic shock
Extracardiac pulmonary causes
1. Bronchial asthma2. Tension pneumothorax
Extracardiac non-pulmonary causes
1. Anaphylactic shock (during urokinase administration) 2. Volvulus of the stomach3. Diaphragmatic hernia4. Superior vena cava obstruction5. Extreme obesity
Mechanism
There is no consensus on the underlying mechanism of pulsus paradoxus.
The major theories proposed for the mechanism in cardiac tamponade and constrictive pericarditis have included:
1. Limited transmission of negative intrathoracic pressure to intrapericardial structures compared with the extrapericardial veins, resulting in loss of the pressure gradient for cardiac filling (“impaired pressure transmission”);
2. Pooling of blood in the pulmonary vasculature during inspiration as a result of increased pulmonary venous compliance, leading to decreased left ventricular filling (“pulmonary venous pooling”);
3.Impaired filling of the left ventricle due to inspiratory filling of the right heart in a constricted pericardial space (“ventricular diastolic interdependence”); , the right ventricle distends due to increased venous return, the interventricular septum bulges into the left ventricle reducing its size (hence the name “reversed Bernheim effect”), and increased pooling on blood in the expanded lungs decreases return to the left ventricle, decreasing the stroke volume of the left ventricle.
4. Constraint of cardiac filling due to inspiratory deformation of the pericardium (“pericardial tug”);
5.Increased respiratory variability in systemic venous return in cardiac tamponade (“systemic venous return variation”).
6. Increased impedance to left ventricular ejection from negative pleural pressure (“afterload theory”);
7. Ventricular septal flattening causes impaired left ventricular systolic function (“ventricular systolic interdependence”).
8. In exacerbations of asthma and COPD, the exaggerated swings in pleural pressure may enhance the normal respiratory variation in venous return through the mechanisms discussed. In addition, hyperinflation of the lungs in these conditions may also impede right ventricular ejection causing decreased filling of the left ventricle (“pulmonary
afterload”).
What is reverse pulsus paradoxus?
Reversed pulsus paradoxus, a rise in systolic blood pressure during inspiration, was first described by Massumi et al, in patients with idiopathic hypertrophic subaortic stenosis, isorhythmic ventricular rhythm and patients of left ventricular failure on positive pressure ventilation. A rise in peak systolic pressure on inspiration by more than 15 mm Hg is considered significant. In a mechanically ventilated patient, positive pressure ventilation displaces the ventricle wall inward during systole to assist in ventricular emptying causing a slight rise in the systolic pressure during mechanical inspiration. A reverse pulsus paradoxus in mechanically ventilated patients is a sensitive indicator of hypovolaemia.
Pseudo pulsus paradoxus
Salel et al described a patient of complete heart block who was misdiagnosed to have pulsus paradoxus. This was the result of forfituous synchronism of inspiration with the cyclic intermittent properly timed atrial contribution to ventricular filling characteristic of atrioventricular dissociation in this condition. This is termed pseudopulsus paradoxus. This error can be avoided by strictly adhering to the guidelines for pulsus paradoxus laid down by Gauchat and Katz: (1) The pulse must be felt in all the accessible arteries (2) There is no need for deep inspiration and (3) There must be no irregularity of cardiac action.
Causes of absent pulsus paradoxus in expected diseases
All cases of cardiac tamponade are not accompanied by pulsus paradoxus. The reasons for this are not clear in all cases, but it is likely that other compensatory mechanisms are brought into play in order to maintain a normal systemic blood pressure. The following are such conditions:
1. Aortic regurgitation (AR): In the presence of AR, the left ventricle can fill from the aorta during inspiration. Therefore, if aortic dissection produces both AR and tamponade, pulsus paradoxus may be absent.
2. Large atrial septal defect: The normal increase in systemic venous return on inspiration is balanced by a decrease in the left to right shunt, resulting in minimal change in the right ventricular volume.
3. Isolated right heart tamponade: This entity has been described in patients of chronic renal failure on hemodialysis.
4. Elevated left ventricular diastolic pressures.
5. Severe rheumatoid spondylitis or disease of the bony thorax: Wide changes in intrathoracic pressure prevented by the relative immobility of the chest wall.
6. Coexistent condition producing “reversed pulsus paradoxus”.
Importance of kussumals sign in pulsus paradoxus
Kussmaul’s sign is a paradoxical increase in the peripheral venous distension and pressure during inspiration. The major mechanism is a change in the shape of the pericardium with a resulting increase in the intrapericardial pressure and obstruction to the venous return to the heart. Compare this with the marked exaggeration of the normal expiratory increase in venous pressure that accompanies patients with pulmonary disease. Note that pulsus paradoxus may be present in both groups of patients.
References
1. Lambert A. Wu , M.D et al. n engl j med 349;7, august 14, 2003.
2. Kussmaul A, Stern Mt. Pericarditis and the paradox pulse. Berl Klin Wochenschr 1873: 38.
3. Katz L N, Gauchat HW. Observations on pulsus paradoxus (with special reference to
pericardial effusions). Arch Intern Med 1924; 33: 371–93.
4. Khasnis A, Lokhandwala Y;JPGM;Year : 2002 ,Volume : 48 , Issue : 1 , Page : 46-9.
5. Kenneth C Bilchick, Robert A Wise; THE LANCET • Vol 359 • June 1, 2002
( Special thanks to Dr. Ajit Babu, Prof. of Medicine AIMS,Cochin for his valuable corrections on this articles based on which a few corrections and references being added)
The simplest definition of pulsus paradoxus is an exaggeration of the normal inspiratory decrease in systolic blood pressure. The current formal definition of pulsus paradoxus is an inspiratory fall of systolic blood pressure of greater than 10 mm Hg.
History
The reduction in pulse volume during inspiration was first described by Lomer in 1669 in constrictive pericarditis. A similar finding was described by Floyer and later by William in 1850 in bronchial asthma. Adolf Kussmaul (Freiberg, Germany) coined the term “pulsus paradoxus” in 1873 in three patients with constrictive pericarditis .Adolf Kussmaul in his 1873 manuscript ‘Ueber schwielge mediastinopericarditis und den paradoxen puls’ (Constrictive Pericarditis and the paradoxical pulse; ) described two important physical signs of pericardial disease: pulsus paradoxus and Kussmaul’s sign.
What is the paradox?
The paradox described by Kussmaul was a “pulse simultaneously slight and irregular, disappearing during inspiration and returning upon expiration” despite the continued presence of the cardiac impulse during both respiratory phases.
Others has described additional paradoxus in the same phenomenon that amidst the irregulary of the pulse palpated, the regularity with which the pulse disappeared during inspiration Moreover, another paradoxus was that the clinical method of assessment of this “pulse” is by measurement of the “systolic blood pressure”.
Methods of examination
1.Palpation(Clinical) :Usually, palpation of the central pulses (carotid) is recommended for the evaluation of the character of the pulse. However, pulsus paradoxus is better appreciated in the peripheral pulses (radial). When the pulsus paradoxus is severe, it may be possible to palpate a fall (reduction in the pulse volume) during the phase of inspiration and rise during the expiratory phase.
2.By Sphygmomanometer(Clinical): To measure the inspiratory decrease in systolic blood pressure, the cuff is first inflated 20 mm Hg above the systolic pressure, then deflated until the first Korotkoff sound is heard. Initially the Korotkoff sounds are heard only during expiration. The cuff is deflated until the Korotkoff sounds are heard equally well during inspiration and expiration. The pressure at which all the Korotkoff sounds are heard should be subtracted from the systolic pressure. If the difference between these two pressures is greater than 10 mm Hg, the patient has a pulsus paradoxus of a magnitude equal to that difference.
3.Pulse oximetry waveform analysis This technique has been found useful in the neonates with cardiac tamponade. In patients with obstructive airway disease since pulse oximetry is available in ICUs and emergency departments, it is a useful non-invasive means of continually assessing pulsus paradoxus and air trapping severity.
4.Arterial waveform analysisIn the intensive care setting, where the arterial waveform is available, pulsus paradoxus can be diagnosed by visualising changes in the systolic blood pressure tracing during the inspiratory and expiratory phases of respiration.
Causes of Pulsus Paradoxus
Cardiac causes
1. Cardiac tamponade2. Pericardial effusion3. Constrictive pericarditis4. Restrictive cardiomyopathy5. Pulmonary embolism6. Acute myocardial infarction7. Cardiogenic shock
Extracardiac pulmonary causes
1. Bronchial asthma2. Tension pneumothorax
Extracardiac non-pulmonary causes
1. Anaphylactic shock (during urokinase administration) 2. Volvulus of the stomach3. Diaphragmatic hernia4. Superior vena cava obstruction5. Extreme obesity
Mechanism
There is no consensus on the underlying mechanism of pulsus paradoxus.
The major theories proposed for the mechanism in cardiac tamponade and constrictive pericarditis have included:
1. Limited transmission of negative intrathoracic pressure to intrapericardial structures compared with the extrapericardial veins, resulting in loss of the pressure gradient for cardiac filling (“impaired pressure transmission”);
2. Pooling of blood in the pulmonary vasculature during inspiration as a result of increased pulmonary venous compliance, leading to decreased left ventricular filling (“pulmonary venous pooling”);
3.Impaired filling of the left ventricle due to inspiratory filling of the right heart in a constricted pericardial space (“ventricular diastolic interdependence”); , the right ventricle distends due to increased venous return, the interventricular septum bulges into the left ventricle reducing its size (hence the name “reversed Bernheim effect”), and increased pooling on blood in the expanded lungs decreases return to the left ventricle, decreasing the stroke volume of the left ventricle.
4. Constraint of cardiac filling due to inspiratory deformation of the pericardium (“pericardial tug”);
5.Increased respiratory variability in systemic venous return in cardiac tamponade (“systemic venous return variation”).
6. Increased impedance to left ventricular ejection from negative pleural pressure (“afterload theory”);
7. Ventricular septal flattening causes impaired left ventricular systolic function (“ventricular systolic interdependence”).
8. In exacerbations of asthma and COPD, the exaggerated swings in pleural pressure may enhance the normal respiratory variation in venous return through the mechanisms discussed. In addition, hyperinflation of the lungs in these conditions may also impede right ventricular ejection causing decreased filling of the left ventricle (“pulmonary
afterload”).
What is reverse pulsus paradoxus?
Reversed pulsus paradoxus, a rise in systolic blood pressure during inspiration, was first described by Massumi et al, in patients with idiopathic hypertrophic subaortic stenosis, isorhythmic ventricular rhythm and patients of left ventricular failure on positive pressure ventilation. A rise in peak systolic pressure on inspiration by more than 15 mm Hg is considered significant. In a mechanically ventilated patient, positive pressure ventilation displaces the ventricle wall inward during systole to assist in ventricular emptying causing a slight rise in the systolic pressure during mechanical inspiration. A reverse pulsus paradoxus in mechanically ventilated patients is a sensitive indicator of hypovolaemia.
Pseudo pulsus paradoxus
Salel et al described a patient of complete heart block who was misdiagnosed to have pulsus paradoxus. This was the result of forfituous synchronism of inspiration with the cyclic intermittent properly timed atrial contribution to ventricular filling characteristic of atrioventricular dissociation in this condition. This is termed pseudopulsus paradoxus. This error can be avoided by strictly adhering to the guidelines for pulsus paradoxus laid down by Gauchat and Katz: (1) The pulse must be felt in all the accessible arteries (2) There is no need for deep inspiration and (3) There must be no irregularity of cardiac action.
Causes of absent pulsus paradoxus in expected diseases
All cases of cardiac tamponade are not accompanied by pulsus paradoxus. The reasons for this are not clear in all cases, but it is likely that other compensatory mechanisms are brought into play in order to maintain a normal systemic blood pressure. The following are such conditions:
1. Aortic regurgitation (AR): In the presence of AR, the left ventricle can fill from the aorta during inspiration. Therefore, if aortic dissection produces both AR and tamponade, pulsus paradoxus may be absent.
2. Large atrial septal defect: The normal increase in systemic venous return on inspiration is balanced by a decrease in the left to right shunt, resulting in minimal change in the right ventricular volume.
3. Isolated right heart tamponade: This entity has been described in patients of chronic renal failure on hemodialysis.
4. Elevated left ventricular diastolic pressures.
5. Severe rheumatoid spondylitis or disease of the bony thorax: Wide changes in intrathoracic pressure prevented by the relative immobility of the chest wall.
6. Coexistent condition producing “reversed pulsus paradoxus”.
Importance of kussumals sign in pulsus paradoxus
Kussmaul’s sign is a paradoxical increase in the peripheral venous distension and pressure during inspiration. The major mechanism is a change in the shape of the pericardium with a resulting increase in the intrapericardial pressure and obstruction to the venous return to the heart. Compare this with the marked exaggeration of the normal expiratory increase in venous pressure that accompanies patients with pulmonary disease. Note that pulsus paradoxus may be present in both groups of patients.
References
1. Lambert A. Wu , M.D et al. n engl j med 349;7, august 14, 2003.
2. Kussmaul A, Stern Mt. Pericarditis and the paradox pulse. Berl Klin Wochenschr 1873: 38.
3. Katz L N, Gauchat HW. Observations on pulsus paradoxus (with special reference to
pericardial effusions). Arch Intern Med 1924; 33: 371–93.
4. Khasnis A, Lokhandwala Y;JPGM;Year : 2002 ,Volume : 48 , Issue : 1 , Page : 46-9.
5. Kenneth C Bilchick, Robert A Wise; THE LANCET • Vol 359 • June 1, 2002
( Special thanks to Dr. Ajit Babu, Prof. of Medicine AIMS,Cochin for his valuable corrections on this articles based on which a few corrections and references being added)
Tuesday, April 25, 2006
Thought of the week: NHS reforms and its impact on Indian doctors in UK
In 1963 the Conservative Health Minister Enoch Powell launched a campaign to recruit Indian doctors to save the NHS from an impending staffing crisis. Ironically, a few years later Powell warned Britain of the “rivers of blood” caused by the influx of foreign workers. By the mid-sixties more than 18,000 doctors had arrived in Britain. Most of them dreamt of working in advanced teaching hospitals. But there was a shock waiting for them.
They were shepherded to either crime and unemployment ridden inner city areas or the small rural communities, where English doctors were reluctant to go.
Last week, York Hospitals NHS Trust decided to cut 200 jobs over the coming year as part of plans to save seven million pounds. Two days earlier the Worcestershire Acute Hospitals NHS Trust had announced that 720 jobs were to be axed as it tries to save 30 million pounds.The University Hospital of North Staffordshire is cutting 1,000 jobs in the face of a 15.5 million pound debt, while Brighton and Sussex University Hospitals NHS Trust is also losing 325 posts as part of plans to save more than 10 million pounds over the next year.The Royal Free Hospital in Hampstead, north London, is cutting about 480 jobs under plans to save 25 million pounds in the next year, and the Mid Cheshire Hospitals NHS Trust said that it could be forced to cut 250 jobs to avoid going into debt.To save costs, some hospitals - such as those in Staffordshire - have resorted to outsourcing medical secretarial work to India. A similar pilot scheme at the Royal Cornwall Hospital (RCH) has been opposed by the local staff.As one of the cost-cutting schemes, hospital officials have proposed that consultants use a digital recorder to dictate notes that can be uploaded via the internet and sent to companies in India and elsewhere to be typed.A spokesman for RCH said: "We are reviewing ways to address a backlog of work that cannot be met, at the moment, by staff at the trust. We are considering companies who provide similar services for other NHS organisations and throughout any pilots they will be monitored and assessed on their speed of turnaround, accuracy, reliability and cost issues. We will then evaluate the outcomes."
Almost every day, several hospitals announce job cuts to meet budget deficits. In recent weeks, the overall job losses in the NHS are said to be nearly 7,000 in 22 trusts and hospitals in different parts of the country.The financial crunch further lessens the prospects of thousands of Indian doctors currently seeking employment in Britain. New work rules have compounded the situation for them as now they can no longer work as part of "permit free training", and need work permits.Britain's health authorities are faced with higher numbers of local medical graduates and many more from the expanded European Union who have the right to work in Britain. The situation makes it difficult for non-EU nationals - such as Indian doctors - to secure employment in the NHS.An association of doctors of Indian origin has scheduled a demonstration outside the Department of Health here April 21 to protest against the changes in work rules as applicable to Indian doctors.
Thousands of Indian and other foreign doctors are forced to live on the breadline in UK because they are lured from their home countries with promises of work, only to remain unemployed, poor and discriminated against a year after expensively gaining UK visas and pass grades in a key medical exam. The new survey, by the General Medical Council, UK’s lead medical body, comes a year after the British Medical Journal published data, case studies and statistics to warn overseas doctors—particularly from India—to eschew UK as they were at risk of remaining out of work for months on end. The GMC survey, which renews the warning, offers data to prove that less than half of those who passed Britain’s medical qualifications test, PLAB, in summer 2004 found work within six months. The survey found that a quarter of those who passed the PLAB or professional and linguistic assessment board, remained down and out in London and other British cities a year later. The survey warned that the situation was likely to worsen in 2006 with nearly 7,000 non-European doctors rushing to pass the PLAB in 2005, up nearly seven times from the 1,000 doctors who passed the test in 1998. The GMC, which administers the PLAB, admitted that the race to clear the exam, mostly amongst doctors from the sub-continent, was prompted by an attempt to recruit overseas, non-European doctors to plug gaps in National Health Service. The department of health said it was considering allowing overseas doctors to apply for jobs from their home countries, a longterm key request by British Indian doctors. Last February, the BMJ “warning to all junior overseas doctors” carried well-chosen words of advice from Peter Trewby, chair of the Royal College of Physicians’ working group on international medical graduates, with the stark facts about the life an Indian doctor could expect in the UK. Recounting the stark fact that a whopping 900, mainly Indian, applicants had attempted to secure the unglamorous post of “a preregistration house officer in Darlington”, Trewby declared the unsuccessful majority of applicants constituted a massive waste of human resource totaling 800 “doctor years”. Senior British Indian doctors told TOI that the faultline appeared to lie in the NHS’s attempt to recruit internationally from September 2001, with the aim of bringing in 1,000 senior doctors and thousands of nurses from overseas into the UK within four years. They said the UK’s policy of declaring healthcare a “skills shortage occupation” gave Indian doctors both the licence and hopes of securing jobs in Britain with the result that “over two-thirds of doctors registering to practise in the UK in 2003 were from overseas—the vast majority from non-European countries”. But the reality of life in UK for a newly-qualified Indian doctor now means queuing for free meals in temples and sleeping three to a room in squalid lodgings, the survey said. In response to the survey, Prasada Rao, BIDA chairman and a general practitioner, said the figures were “absolutely diabolical… unbelievable. These people have come to serve NHS and there is chaos, confusion and total lack of care. There is no co-ordination between the health department, home office and GMC. It is totally unacceptable.”"
Why are the Indian doctors forced to leave their home land and work in UK and Canada and the land of downunders Australia. Only because of poor work atmosphere at home,the meagre salaries , the focus on curative treatment and gross negligence of scientific research and lack of direction from the part of policy makers who are bend on bribery and corruption. Inspite of gross defecits of GP's and Physicians in the rural india where you are offered handsome salaries as per indian standards, almost all the doctors and consultants are crowded in cities there by decrasing the relative job deficit in cities amounting to low salaries and exploitations from the part of private hospitals who try to keep the salaries of thedoctors at the rock bottom. Service part of the profession is lost to big corporates who rule the health care and inluence the policy making to make inappropriate profit and loot both the health professionals as well as the patients.
What is now needed is developing a central INHS for india, Posting of fresh MBBS graduates in rural india with good salaries and limiting their work time, with a proper referral system, to abolish undue importance to superspecialists , reduce the duration of MBBS,MD and DM courses and the governmental assistance in recruitment of doctors to foreign countries especially to Australia and CANADA where the deficits of health professionals are increasing. Making compulsory insurance for the masses and restricting the private hopitals and setting a bench mark salary will defenitely solve the problem of employment among doctors. Setting up of newer and newer self financing colleges is ruining the whole scenario and needs immediate restrictions or else the same doom in UK is sure to fall on us too.
Editor's desk
They were shepherded to either crime and unemployment ridden inner city areas or the small rural communities, where English doctors were reluctant to go.
Last week, York Hospitals NHS Trust decided to cut 200 jobs over the coming year as part of plans to save seven million pounds. Two days earlier the Worcestershire Acute Hospitals NHS Trust had announced that 720 jobs were to be axed as it tries to save 30 million pounds.The University Hospital of North Staffordshire is cutting 1,000 jobs in the face of a 15.5 million pound debt, while Brighton and Sussex University Hospitals NHS Trust is also losing 325 posts as part of plans to save more than 10 million pounds over the next year.The Royal Free Hospital in Hampstead, north London, is cutting about 480 jobs under plans to save 25 million pounds in the next year, and the Mid Cheshire Hospitals NHS Trust said that it could be forced to cut 250 jobs to avoid going into debt.To save costs, some hospitals - such as those in Staffordshire - have resorted to outsourcing medical secretarial work to India. A similar pilot scheme at the Royal Cornwall Hospital (RCH) has been opposed by the local staff.As one of the cost-cutting schemes, hospital officials have proposed that consultants use a digital recorder to dictate notes that can be uploaded via the internet and sent to companies in India and elsewhere to be typed.A spokesman for RCH said: "We are reviewing ways to address a backlog of work that cannot be met, at the moment, by staff at the trust. We are considering companies who provide similar services for other NHS organisations and throughout any pilots they will be monitored and assessed on their speed of turnaround, accuracy, reliability and cost issues. We will then evaluate the outcomes."
Almost every day, several hospitals announce job cuts to meet budget deficits. In recent weeks, the overall job losses in the NHS are said to be nearly 7,000 in 22 trusts and hospitals in different parts of the country.The financial crunch further lessens the prospects of thousands of Indian doctors currently seeking employment in Britain. New work rules have compounded the situation for them as now they can no longer work as part of "permit free training", and need work permits.Britain's health authorities are faced with higher numbers of local medical graduates and many more from the expanded European Union who have the right to work in Britain. The situation makes it difficult for non-EU nationals - such as Indian doctors - to secure employment in the NHS.An association of doctors of Indian origin has scheduled a demonstration outside the Department of Health here April 21 to protest against the changes in work rules as applicable to Indian doctors.
Thousands of Indian and other foreign doctors are forced to live on the breadline in UK because they are lured from their home countries with promises of work, only to remain unemployed, poor and discriminated against a year after expensively gaining UK visas and pass grades in a key medical exam. The new survey, by the General Medical Council, UK’s lead medical body, comes a year after the British Medical Journal published data, case studies and statistics to warn overseas doctors—particularly from India—to eschew UK as they were at risk of remaining out of work for months on end. The GMC survey, which renews the warning, offers data to prove that less than half of those who passed Britain’s medical qualifications test, PLAB, in summer 2004 found work within six months. The survey found that a quarter of those who passed the PLAB or professional and linguistic assessment board, remained down and out in London and other British cities a year later. The survey warned that the situation was likely to worsen in 2006 with nearly 7,000 non-European doctors rushing to pass the PLAB in 2005, up nearly seven times from the 1,000 doctors who passed the test in 1998. The GMC, which administers the PLAB, admitted that the race to clear the exam, mostly amongst doctors from the sub-continent, was prompted by an attempt to recruit overseas, non-European doctors to plug gaps in National Health Service. The department of health said it was considering allowing overseas doctors to apply for jobs from their home countries, a longterm key request by British Indian doctors. Last February, the BMJ “warning to all junior overseas doctors” carried well-chosen words of advice from Peter Trewby, chair of the Royal College of Physicians’ working group on international medical graduates, with the stark facts about the life an Indian doctor could expect in the UK. Recounting the stark fact that a whopping 900, mainly Indian, applicants had attempted to secure the unglamorous post of “a preregistration house officer in Darlington”, Trewby declared the unsuccessful majority of applicants constituted a massive waste of human resource totaling 800 “doctor years”. Senior British Indian doctors told TOI that the faultline appeared to lie in the NHS’s attempt to recruit internationally from September 2001, with the aim of bringing in 1,000 senior doctors and thousands of nurses from overseas into the UK within four years. They said the UK’s policy of declaring healthcare a “skills shortage occupation” gave Indian doctors both the licence and hopes of securing jobs in Britain with the result that “over two-thirds of doctors registering to practise in the UK in 2003 were from overseas—the vast majority from non-European countries”. But the reality of life in UK for a newly-qualified Indian doctor now means queuing for free meals in temples and sleeping three to a room in squalid lodgings, the survey said. In response to the survey, Prasada Rao, BIDA chairman and a general practitioner, said the figures were “absolutely diabolical… unbelievable. These people have come to serve NHS and there is chaos, confusion and total lack of care. There is no co-ordination between the health department, home office and GMC. It is totally unacceptable.”"
Why are the Indian doctors forced to leave their home land and work in UK and Canada and the land of downunders Australia. Only because of poor work atmosphere at home,the meagre salaries , the focus on curative treatment and gross negligence of scientific research and lack of direction from the part of policy makers who are bend on bribery and corruption. Inspite of gross defecits of GP's and Physicians in the rural india where you are offered handsome salaries as per indian standards, almost all the doctors and consultants are crowded in cities there by decrasing the relative job deficit in cities amounting to low salaries and exploitations from the part of private hospitals who try to keep the salaries of thedoctors at the rock bottom. Service part of the profession is lost to big corporates who rule the health care and inluence the policy making to make inappropriate profit and loot both the health professionals as well as the patients.
What is now needed is developing a central INHS for india, Posting of fresh MBBS graduates in rural india with good salaries and limiting their work time, with a proper referral system, to abolish undue importance to superspecialists , reduce the duration of MBBS,MD and DM courses and the governmental assistance in recruitment of doctors to foreign countries especially to Australia and CANADA where the deficits of health professionals are increasing. Making compulsory insurance for the masses and restricting the private hopitals and setting a bench mark salary will defenitely solve the problem of employment among doctors. Setting up of newer and newer self financing colleges is ruining the whole scenario and needs immediate restrictions or else the same doom in UK is sure to fall on us too.
Editor's desk
Monday, April 24, 2006
ECG zone: Sgarbossa's Criteria: Not just another criteria
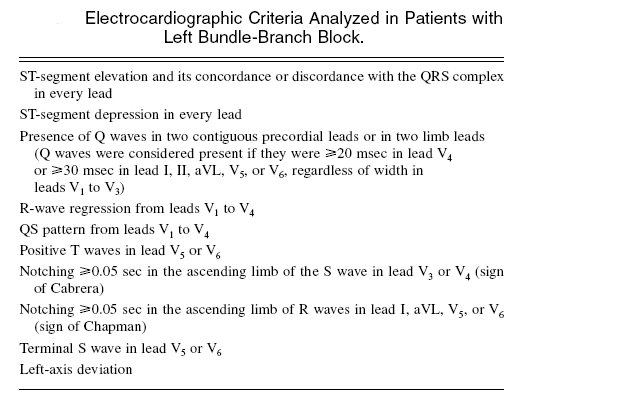
The presence of left bundlebranch block on the electrocardiogram may conceal the changes of acute myocardial infarction, which can delay both its recognition and thrombolytic treatment. Elena.B.Sgarbossa et al tested electrocardiographic criteria for the diagnosis of acute infarction in the presence of left bundle-branch block in patients enrolled in the GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) trial who had left bundle-branch block and acute myocardial infarction confirmed by enzyme studies were blindly compared with the electrocardiograms of control patients who had chronic coronary artery disease and left bundle-branch block. The criteria studied is given in the table below. They found that ST-segment deviation was the only electrocardiographic finding that was useful in the diagnosis of acute myocardial infarction in the presence of left bundle-branch block. Previously proposed electrocardiographic signs involving the QRS complex were not useful.
The ST changes that were significant are:
1.ST elevation > or = 1mm and concordant with QRS.
2.ST depression > or = 1mm in v1,v2 or v3.
3.ST elevation > or = 5mm and discordant with QRS.
For a CME go to mcqs-online.blogspot.com or click on the link in side bar.
References:
1. Elena.B.Sgarbossa et al; New England Journal of Medicine, Volume 334 ;Number 8, FEBRUARY 22, 1996.
Web trawl
Editor’s notes: Ever wondered about the numerous clinical signs of aortic regurgitations, which the examiners and your colleges are so fond of. Never seen them in "standard " clinical textbooks and their mechanisms poorly described by its ardent followers, even though widely revered. Are they clinically and scientifically correct. The following article in Annals of Internal medicine may help you. If interested in reading the full article you may contact the editor’s email..................
Eponyms and the Diagnosis of Aortic Regurgitation:
What Says the Evidence?
Ajit N. Babu, MBBS, MPH; Steven M. Kymes, PhD, MHA; and Sharon M. Carpenter Fryer, MS, RD
Background: Chronic aortic regurgitation can lead to significant
morbidity and mortality. For more than a century, numerous eponymous
signs of aortic regurgitation have been described in textbooks
and the literature.
Purpose: To compare current textbook content with the peerreviewed
literature on the eponymous signs of aortic regurgitation
and to assess the role of these signs in clinical practice.
Data Sources: 11 textbooks, MEDLINE (1966 through October
2002), and bibliographies of textbooks and relevant papers.
Study Selection: English-language reports that were related to
the properties of a sign on physical examination, incorporated
more than 10 adults, and did not involve prosthetic heart valves or
acute aortic regurgitation.
Data Extraction: Three investigators independently analyzed
relevant textbook extracts and 27 reports, using predetermined
qualitative review criteria. Data relating to diagnostic accuracy and
properties of the index test were also extracted.
Data Synthesis: Twelve eponymous signs were described as
having varying degrees of importance by textbook authors. Only
the Austin Flint murmur, the Corrigan pulse, the Duroziez sign,
and the Hill sign had sufficient original literature for detailed
review. Most reports were low quality, with varying sensitivities
for all signs. Except for the Hill sign, specificity tended to be poor.
Evidence for the Hill sign also suggested a correlation between the
popliteal–brachial gradient and aortic regurgitation severity.
Conclusions: Prominent textbook support of the eponymous
signs of aortic regurgitation is not matched by the literature.
Clinicians and educators should update and improve the evidence
for these signs to ensure their relevance in current medical practice.
Ann Intern Med. 2003;138:736-742. www.annals.org
Eponyms and the Diagnosis of Aortic Regurgitation:
What Says the Evidence?
Ajit N. Babu, MBBS, MPH; Steven M. Kymes, PhD, MHA; and Sharon M. Carpenter Fryer, MS, RD
Background: Chronic aortic regurgitation can lead to significant
morbidity and mortality. For more than a century, numerous eponymous
signs of aortic regurgitation have been described in textbooks
and the literature.
Purpose: To compare current textbook content with the peerreviewed
literature on the eponymous signs of aortic regurgitation
and to assess the role of these signs in clinical practice.
Data Sources: 11 textbooks, MEDLINE (1966 through October
2002), and bibliographies of textbooks and relevant papers.
Study Selection: English-language reports that were related to
the properties of a sign on physical examination, incorporated
more than 10 adults, and did not involve prosthetic heart valves or
acute aortic regurgitation.
Data Extraction: Three investigators independently analyzed
relevant textbook extracts and 27 reports, using predetermined
qualitative review criteria. Data relating to diagnostic accuracy and
properties of the index test were also extracted.
Data Synthesis: Twelve eponymous signs were described as
having varying degrees of importance by textbook authors. Only
the Austin Flint murmur, the Corrigan pulse, the Duroziez sign,
and the Hill sign had sufficient original literature for detailed
review. Most reports were low quality, with varying sensitivities
for all signs. Except for the Hill sign, specificity tended to be poor.
Evidence for the Hill sign also suggested a correlation between the
popliteal–brachial gradient and aortic regurgitation severity.
Conclusions: Prominent textbook support of the eponymous
signs of aortic regurgitation is not matched by the literature.
Clinicians and educators should update and improve the evidence
for these signs to ensure their relevance in current medical practice.
Ann Intern Med. 2003;138:736-742. www.annals.org
Sunday, April 23, 2006
X ray corner and Quiz zone

Case Report: Idiopathic hypoparathyroidism presenting as Secondary myelofibrosis : A rare disease association.
Dr.Jithesh.K. PG student calicut medical college*
Prof.P.K. Sasidharan; Dept. of General medicine calicut medical college**
(*=First author;**=Second author)
Key words
Myelofibrosis , Idiopathic hypoparathyroidism , Secondary Myelofibrosis.
Abstract
Myelofibrosis occurring both in childhood and adulthood is most commonly idiopathic, followed by neoplastic infiltration of the bone marrow. We are reporting an extremely rare association of Idiopathic hypoparathyroidism associated with stable secondary Myelofibrosis.
Introduction
Myelofibrosis or fibrosis (MF) of bone marrow is an uncommon condition in children. Fewer than 100 cases of myelofibrosis in children have been described in medical literature 1 . Most cases in children arise secondary to other disease processes. In adults it is not a rare disorder but most cases are idiopathic and if secondary, they are mostly due to neoplastic infiltration of bone marrow. Secondary causes in the adults include infections, carcinomatous metastases to the marrow, Hodgkin’s and Non Hodgkin’s lymphomas, Chronic Myeloid leukemia, Hairy cell Leukemia, Polycythemia Rubra Vera, SLE, Systemic mastocytosis etc.2. We are reporting an extremely rare association of Idiopathic hypoparathyroidism with stable and untreated Myelofibrosis in an adult patient on treatment from the age of 9 years with a diagnosis of Indian Childhood Cirrhosis, which was probably a wrong diagnosis.
Case Report
29-year-old mentally challenged female was admitted in our ward with insidious and progressive upper abdominal distention with easy bruisability, bleeding from gums and ecchymosis since childhood. Her previous treatment records showed that she was under regular medical treatment with haematinics and repeated fresh blood transfusions for bleeding from gums and echymosis due to thrombocytopenia presumptively due to hypersplenism for past 20 years. Previously she was erroneously treated as a case of Indian childhood cirrhosis and was under regular use of diuretics also for the ascites. Recently she presented with easy bruising and on evaluation she was found to have pancytopenia as per her complete haemogram Hb – 6.4 gm/dl ,TC – 3,800 cell/mm3 , DC – P72 L 28 , Platelet count – 48,000/mm3 , MCV-78.5 fl,MCH - 29.3 pg, MCHC- 24 gm/dl , ESR – 34mm/I hour thought to be due to hyperspelnism. The bone marrow biopsy done during the work up for pancytopenia, in our department, showed hyperplasic phase of myelofibrosis. The cause of myelofibrosis was considered to be due to secondary cause in view of her age and onset of symptoms since childhood and a detailed evaluation for various secondary causes for myelofibrosis was done. Her family history was not contributory . On examination , there was facial dysmorphism with prominent malars , pinched up nose and narrow upper lip ( Figure)
Her hands showed abnormal dermatoglyphics with clinodactyly of the little fingers.
There was extensive caries of teeth with malocclusion in spite of a good oral hygiene and absence of gingivitis (Figure 4)
She was short statured and was having genu valgum and pes planus (Figure 5)
Abdomen showed massive splenomegaly with asymmetrically enlarged liver and ascites. Repeat haemogram also showed pancytopenia.
Bone marrow trephine biopsy showed hyperplastic phase of myelofibrosis (Figure 6) and peripheral smear showed teardrop cells. Because of the skeletal abnormalities and caries teeth and also because of the mention of hypoparathyroidism as a cause for myelofibrosis in medical literature, we wanted to rule out that, or another disorder of calcium homeostasis, though she had no symptoms or signs of hypocalcaemia. Serum calcium was 7.8 mg/dl, serum phosphate was 11.4 mg/dl and alkaline phosphatase was 124 IU/ml with normal renal function tests, which suggested the possibility of hypoparathyroidism . PTH assay was done which was 6.5 ngm/ml ( Normal :9-15 ngm/ml ) with TmP / GFR of 1.4mmol/L which confirmed primary hypoparathyroidism . Radiological survey of skeletal system did not show any features of extra skeletal calcifications . USG abdomen showed massive splenomegaly with liver echogenicity suggestive of cirrhosis. Liver biopsy or further studies to evaluate the cause of hepatosplenomegaly was not possible in this patient considering the risk of bleeding due to thrombocytopenia, her poor general condition and the unwillingness of parents for such procedures. Cirrhosis in this patient with Myelofibrosis was due to the chronic presentation of Budd chiari syndrome. The association of Chronic Budd chiari syndrome with Myelofibrosis is well established and reported and probably due to the extramedullary haematopoesis occurring in the liver. The possibility of transfusion associated chronic viral hepatitis by HBV and HCV has been excluded by viral marker studies and serum ferritin and transferrin levels were within the normal range. Again the possibility of cirrhosis as suggested by the radiologist USG might be a misinterpretation of the nodularity seen in liver echogenicity by the ectopic haemopoetic tissue in liver.
Ascitic fluid study showed a transudate fluid with a SAAG of 1.6. Subsequently the patient was put on calcium supplementation along with 1,25 dihydroxycholecalciferol and Calcium carbonate as calcium supplement and as phosphate binder, and is under follow up.
Discussion
We are reporting this case to draw attention to the rare clinical association of Idiopathic hypoparathyroidism with Myelofibrosis3. Only a single reported case was seen indexed in Pubmed. Though the exact mechanism of myelofibrosis in hypoparathyroidism was previously less well described. In the present case report we are attempting to draw the attention towards the intricate relationship of Parathyroid hormone, osteogenesis and the ontogeny of the bone marrow and its stromal compartment, which is derived from the skeletal stem/progenitor cells. The ontogeny of bone marrow and its stromal compartment, which is generated from skeletal stem/progenitor cells, was investigated in vivo and ex vivo by Kuznetsov SA et al 4, in mice expressing constitutively active parathyroid hormone/parathyroid hormone-related peptide receptor (PTH/PTHrP; caPPR) under the control of the 2.3-kb bone-specific mouse Col1A1 promoter/enhancer. The transgene promoted increased bone formation within prospective marrow space, but delayed the transition from bone to bone marrow during growth, the formation of marrow cavities, and the appearance of stromal cell types such as marrow adipocytes and cells supporting hematopoiesis. This phenotype resolved spontaneously over time, leading to the establishment of marrow containing a greatly reduced number of clonogenic stromal cells. Proliferative osteoprogenitors, but not multipotent skeletal stem cells (mesenchymal stem cells), capable of generating a complete heterotopic bone organ upon in vivo transplantation were assayable in the bone marrow of caPPR mice. Thus, PTH/PTHrP signaling is a major regulator of the ontogeny of the bone marrow and its stromal tissue, and of the skeletal stem cell compartment.
From the above study it is clear that disturbances in PTH mediated signaling of PTH/PTHrP receptors have detrimental effects on proper maturation of a functioning bone marrow in addition to disturbances in osteogenesis and osteoid matrix calcification. In the present patient in our case report, idiopathic hypoparathyroidism, which was existent right from birth, as evidenced by the abnormal dentition and genuvarum may be a contributing factor to development of myelofibrosis.
Chronic hypocalcaemia can be asymptomatic which was the case in this patient , the only odd point is the absence of basal ganglia calcifications and cataracts. However the presence of extensive caries teeth inspite of good dental care , with abnormalities of primary and secondary dentitions and presence of genu valgum all points towards a long standing Ca- Po4 metabolic abnormalities .
Although attempts to correct hypocalcaemia and hyperphosphataemia with Calcium and 1,25 dihydroxycholecalcipherol are beneficial, the long-term benefits in this patient are not known. Treatment of hypo parathyroid patients with synthetic parathyroid hormone is controversial and its effectiveness in this patient is questionable as well. The probable outcome of the disease in this patient is not known at present.
References
1. Maj JS, Roslan K, Fic-Sikorska B: ‘Acute myelofibrosis in children: report on two cases’; Acta Haematol Pol 1996; 27(1): 79-84.
2. Manoharan A: ‘Idiopathic myelofibrosis: a clinical review’. ; Int J Hematol 1998 Dec; 68(4): 355-62.
3. Simpson HK, Howden CW, Elliott HL, Thomson TJ; ‘Idiopathic hypoparathyroidism associated with stable untreated myelofibrosis’; Br Med J (Clin Res Ed). 1983 Apr 23; 286(6374): 1316-7.
4. Kuznetsov SA, Riminucci M et al: ‘The interplay of osteogenesis and hematopoiesis: expression of a constitutively active PTH/PTHrP receptor in osteogenic cells perturbs the establishment of hematopoiesis in bone and of skeletal stem cells in the bone marrow’; J Cell Biol. 2004 Dec 20; 167(6): 1113-22.
Prof.P.K. Sasidharan; Dept. of General medicine calicut medical college**
(*=First author;**=Second author)
Key words
Myelofibrosis , Idiopathic hypoparathyroidism , Secondary Myelofibrosis.
Abstract
Myelofibrosis occurring both in childhood and adulthood is most commonly idiopathic, followed by neoplastic infiltration of the bone marrow. We are reporting an extremely rare association of Idiopathic hypoparathyroidism associated with stable secondary Myelofibrosis.
Introduction
Myelofibrosis or fibrosis (MF) of bone marrow is an uncommon condition in children. Fewer than 100 cases of myelofibrosis in children have been described in medical literature 1 . Most cases in children arise secondary to other disease processes. In adults it is not a rare disorder but most cases are idiopathic and if secondary, they are mostly due to neoplastic infiltration of bone marrow. Secondary causes in the adults include infections, carcinomatous metastases to the marrow, Hodgkin’s and Non Hodgkin’s lymphomas, Chronic Myeloid leukemia, Hairy cell Leukemia, Polycythemia Rubra Vera, SLE, Systemic mastocytosis etc.2. We are reporting an extremely rare association of Idiopathic hypoparathyroidism with stable and untreated Myelofibrosis in an adult patient on treatment from the age of 9 years with a diagnosis of Indian Childhood Cirrhosis, which was probably a wrong diagnosis.
Case Report
29-year-old mentally challenged female was admitted in our ward with insidious and progressive upper abdominal distention with easy bruisability, bleeding from gums and ecchymosis since childhood. Her previous treatment records showed that she was under regular medical treatment with haematinics and repeated fresh blood transfusions for bleeding from gums and echymosis due to thrombocytopenia presumptively due to hypersplenism for past 20 years. Previously she was erroneously treated as a case of Indian childhood cirrhosis and was under regular use of diuretics also for the ascites. Recently she presented with easy bruising and on evaluation she was found to have pancytopenia as per her complete haemogram Hb – 6.4 gm/dl ,TC – 3,800 cell/mm3 , DC – P72 L 28 , Platelet count – 48,000/mm3 , MCV-78.5 fl,MCH - 29.3 pg, MCHC- 24 gm/dl , ESR – 34mm/I hour thought to be due to hyperspelnism. The bone marrow biopsy done during the work up for pancytopenia, in our department, showed hyperplasic phase of myelofibrosis. The cause of myelofibrosis was considered to be due to secondary cause in view of her age and onset of symptoms since childhood and a detailed evaluation for various secondary causes for myelofibrosis was done. Her family history was not contributory . On examination , there was facial dysmorphism with prominent malars , pinched up nose and narrow upper lip ( Figure)
Her hands showed abnormal dermatoglyphics with clinodactyly of the little fingers.
There was extensive caries of teeth with malocclusion in spite of a good oral hygiene and absence of gingivitis (Figure 4)
She was short statured and was having genu valgum and pes planus (Figure 5)
Abdomen showed massive splenomegaly with asymmetrically enlarged liver and ascites. Repeat haemogram also showed pancytopenia.
Bone marrow trephine biopsy showed hyperplastic phase of myelofibrosis (Figure 6) and peripheral smear showed teardrop cells. Because of the skeletal abnormalities and caries teeth and also because of the mention of hypoparathyroidism as a cause for myelofibrosis in medical literature, we wanted to rule out that, or another disorder of calcium homeostasis, though she had no symptoms or signs of hypocalcaemia. Serum calcium was 7.8 mg/dl, serum phosphate was 11.4 mg/dl and alkaline phosphatase was 124 IU/ml with normal renal function tests, which suggested the possibility of hypoparathyroidism . PTH assay was done which was 6.5 ngm/ml ( Normal :9-15 ngm/ml ) with TmP / GFR of 1.4mmol/L which confirmed primary hypoparathyroidism . Radiological survey of skeletal system did not show any features of extra skeletal calcifications . USG abdomen showed massive splenomegaly with liver echogenicity suggestive of cirrhosis. Liver biopsy or further studies to evaluate the cause of hepatosplenomegaly was not possible in this patient considering the risk of bleeding due to thrombocytopenia, her poor general condition and the unwillingness of parents for such procedures. Cirrhosis in this patient with Myelofibrosis was due to the chronic presentation of Budd chiari syndrome. The association of Chronic Budd chiari syndrome with Myelofibrosis is well established and reported and probably due to the extramedullary haematopoesis occurring in the liver. The possibility of transfusion associated chronic viral hepatitis by HBV and HCV has been excluded by viral marker studies and serum ferritin and transferrin levels were within the normal range. Again the possibility of cirrhosis as suggested by the radiologist USG might be a misinterpretation of the nodularity seen in liver echogenicity by the ectopic haemopoetic tissue in liver.
Ascitic fluid study showed a transudate fluid with a SAAG of 1.6. Subsequently the patient was put on calcium supplementation along with 1,25 dihydroxycholecalciferol and Calcium carbonate as calcium supplement and as phosphate binder, and is under follow up.
Discussion
We are reporting this case to draw attention to the rare clinical association of Idiopathic hypoparathyroidism with Myelofibrosis3. Only a single reported case was seen indexed in Pubmed. Though the exact mechanism of myelofibrosis in hypoparathyroidism was previously less well described. In the present case report we are attempting to draw the attention towards the intricate relationship of Parathyroid hormone, osteogenesis and the ontogeny of the bone marrow and its stromal compartment, which is derived from the skeletal stem/progenitor cells. The ontogeny of bone marrow and its stromal compartment, which is generated from skeletal stem/progenitor cells, was investigated in vivo and ex vivo by Kuznetsov SA et al 4, in mice expressing constitutively active parathyroid hormone/parathyroid hormone-related peptide receptor (PTH/PTHrP; caPPR) under the control of the 2.3-kb bone-specific mouse Col1A1 promoter/enhancer. The transgene promoted increased bone formation within prospective marrow space, but delayed the transition from bone to bone marrow during growth, the formation of marrow cavities, and the appearance of stromal cell types such as marrow adipocytes and cells supporting hematopoiesis. This phenotype resolved spontaneously over time, leading to the establishment of marrow containing a greatly reduced number of clonogenic stromal cells. Proliferative osteoprogenitors, but not multipotent skeletal stem cells (mesenchymal stem cells), capable of generating a complete heterotopic bone organ upon in vivo transplantation were assayable in the bone marrow of caPPR mice. Thus, PTH/PTHrP signaling is a major regulator of the ontogeny of the bone marrow and its stromal tissue, and of the skeletal stem cell compartment.
From the above study it is clear that disturbances in PTH mediated signaling of PTH/PTHrP receptors have detrimental effects on proper maturation of a functioning bone marrow in addition to disturbances in osteogenesis and osteoid matrix calcification. In the present patient in our case report, idiopathic hypoparathyroidism, which was existent right from birth, as evidenced by the abnormal dentition and genuvarum may be a contributing factor to development of myelofibrosis.
Chronic hypocalcaemia can be asymptomatic which was the case in this patient , the only odd point is the absence of basal ganglia calcifications and cataracts. However the presence of extensive caries teeth inspite of good dental care , with abnormalities of primary and secondary dentitions and presence of genu valgum all points towards a long standing Ca- Po4 metabolic abnormalities .
Although attempts to correct hypocalcaemia and hyperphosphataemia with Calcium and 1,25 dihydroxycholecalcipherol are beneficial, the long-term benefits in this patient are not known. Treatment of hypo parathyroid patients with synthetic parathyroid hormone is controversial and its effectiveness in this patient is questionable as well. The probable outcome of the disease in this patient is not known at present.
References
1. Maj JS, Roslan K, Fic-Sikorska B: ‘Acute myelofibrosis in children: report on two cases’; Acta Haematol Pol 1996; 27(1): 79-84.
2. Manoharan A: ‘Idiopathic myelofibrosis: a clinical review’. ; Int J Hematol 1998 Dec; 68(4): 355-62.
3. Simpson HK, Howden CW, Elliott HL, Thomson TJ; ‘Idiopathic hypoparathyroidism associated with stable untreated myelofibrosis’; Br Med J (Clin Res Ed). 1983 Apr 23; 286(6374): 1316-7.
4. Kuznetsov SA, Riminucci M et al: ‘The interplay of osteogenesis and hematopoiesis: expression of a constitutively active PTH/PTHrP receptor in osteogenic cells perturbs the establishment of hematopoiesis in bone and of skeletal stem cells in the bone marrow’; J Cell Biol. 2004 Dec 20; 167(6): 1113-22.
Special prizes for Quiz
All readers are invited to participate in quiz for exciting prizes and more...................
Issue:1, Volume:1, April 26,2006 (On print)

Review article
Pulsus Paradoxus (Reverse Bernheim's Sign) : All's not well.
Interesting Case
Idiopathic hypoparathyroidism presenting as Secondary Myelofibrosis.
Web Trawl
Clinical signs of Aortic regurgitation : "References please?!".
From The Editor's desk of CMU
Clinical medicine update(CMU), is an attempt to publish a journal on the dying art of physical examination and bed side diagnosis which is being side lined by the gadgetry and laboratory based diagnosis of medical illnesses. CMU will be updated biweekly. It will have a Review article section on a clinical sign or technique of physical examination and their logical interpretations with extensive, reliable and quotable references from medical literature and textbooks. Interesting cases section will have cases send by readers, which will be published if they are send in a printable form to the editor's email address. Radiology section for interesting X rays, CT scans and MRI's.ECG corner for short snippets on ecgs.Web trawl section for online finds and clinically relevant articles on net.Quiz section as a brain teaser. Thought of the week section a philosphical appraisal of recent events in the world related to medicine.Internal medicine post graduates ,undergraduates, practising consultants and academicians will find this journal useful for enhancing their information in clinical medicine and will find that the lacunae of clinical notes being filled. The publisher wishes valuable advices, corrections and criticisms for further improvement of the journal.
Subscribe to:
Comments (Atom)